
By Peter D’Adamo
From n=1
Although almost everyone knows that fingerprint ridge patterns remain constant and unchanging throughout life (which is why they are so useful to law enforcement) even professionals involved in dermatoglyphics research are often unaware of the changeable nature of the actual height of the ridges themselves. There are a series of surprising correlations between changes to the height of the ridge pattern and links to gluten intolerance found in diseases such as celiac and to certain sensitivities to proteins in the diet called lectins.
Ridge height appears to be linked to many of the same cell processes that control glycosylation in the gut. This is the process of attaching sugars to proteins or fats to make ever more complex molecules. Proper ridge height equates with a patent digestive track, while a worn appearance may signal digestive problems. Known as ridge hypoplasia, this is a situation in which the fingerprint ridges are reduced in height, giving them a “worn-off” appearance. These areas of worn off ridges are also covered with an unusual number of fine secondary creases that become visible, producing what are called “white lines.” (1)
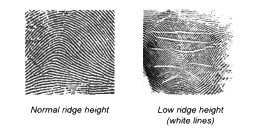
Normal and low ridge height
White lines and celiac disease
Typically, the number of white lines increases with age and with subsequent deterioration of gut integrity. Research dating back to the early 1970’s has linked the appearance of white lines to adults who suffer with celiac disease. (2-6) Ridge height is the only aspect of fingerprints that can actually change with health status. Most interestingly, these white lines often improve with the maintenance of a gluten free diet, and researchers suggest that improvements to ridge height and disappearance of white lines could be used as an indicator of the patient’s response to diet therapy, although complete improvement of the fingerprints could often take as long as two years.
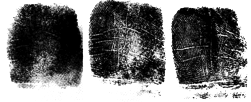
Ridge height of a 54-year-old man with celiac disease
At the left is a series of fingerprint from the right little finger of a 54-year-old man with celiac disease. Left to right: A newly-diagnosed showing almost complete ridge atrophy. Middle: After one-month treatment with gluten free diet. Shows partial ridge atrophy with appearance of white lines. Right: After 11 months on a gluten free diet prints show an almost complete regeneration of the dermal ridges, with disappearance of most white lines. (2)
There is no widespread agreement about the frequency of white lines in the general population. The most extensive study indicated that they are found in the fingerprints of 11-13% of the population, although the study used police records and so would have been made up predominantly of males. (6) Other figures, with broader subject bases, seem to indicate that they can be seen in about 22-30% of all northern Europeans. White lines appear to be more common on the left hand and more commonly on the third and fourth digits. (7-8)
______________________
Image credit: Victor Hugo, ‘Taches with Fingerprints’ (1865)
- D’Adamo PJ. ‘Dermatoglyphics’ in: Fundamentals of Generative Medicine, Volume I. 2010. Drum Hill Books, Wilton CT USA
- Schauman and Alter, Dermatoglyphics in Medical Disorders, Springer Verlag. New York- Heidelberg. 1976
- Mylotte M, Egan-Mitchell B, Fottrell PF, McNicholl B, McCarthy CF. Fingerprints in patients with coeliac disease and their relatives. Br Med J. 1972 Oct 21;4(5833):144-6
- David TJ, Ajdukiewicz AB, Read AE. Dermal and epidermal ridge atrophy in celiac sprue. Gastroenterology. 1973 Apr;64(4):539-44
- David TJ, Ajdukiewicz AB, Read AE. Fingerprint changes in coeliac disease. Br Med J. 1970 Dec 5;4(5735):594-6.
- Cherill FA. Fingerprints and disease. Nature 166: 581. 1950
- Wendt GG. Kranheit in “weisse Linien” der fingerliesten. Artzl. Forsch. 6. 227; 1952 (referenced in 2)
- Wendt GG. Uber weisse im abdruck der menschlichen Fingerbeere. Homo. 6. 180; 1955 (referenced in 2)
