
By Mitchell Bebel Stargrove, ND, LAc and Lori Beth Stargrove, ND
Originally presented as a poster on May 18, 2012 at The International Research Congress on Integrative Medicine and Health 2012
From BMC Complementary and Alternative Medicine 2012;12(Suppl 1):P430.
©2012 Mitchell Bebel Stargrove and Lori Beth Stargrove
INTRODUCTION
In the scientific literature the subject of “interactions” has typically referred to drug-drug interactions. Recently, however herb-drug and drug-nutrient interactions have become an ever-increasing public health concern. Unfortunately the current literature has been poorly representational of these types of interactions. Viewed through a more inclusive paradigm, the subject of “interactions” can play an important role in the emergence of individualized, person-centered healthcare, particularly in the context of aging and the elderly.
As individuals age, they are more likely to suffer from a constellation of health problems, and thus to see multiple healthcare professionals, and be prescribed numerous pharmaceutical medications. Herbal and other nutritional supplements, self-initiated or prescribed, are increasingly popular, and may interact with prescription medications. Polypharmacy may be orchestrated or unsupervised, beneficial or risky. Its effects are dependent upon the individual patient’s physiology, health status and medical condition(s) and the communication and collaboration among the involved healthcare providers. Approached in a proactive manner, the risks and benefits of interactions and polypharmacy can be anticipated and therapies coordinated, thus allowing the practitioner to craft an individualized, predictive and participatory therapeutic strategy with the patient at the center of the care.
DESCRIPTION
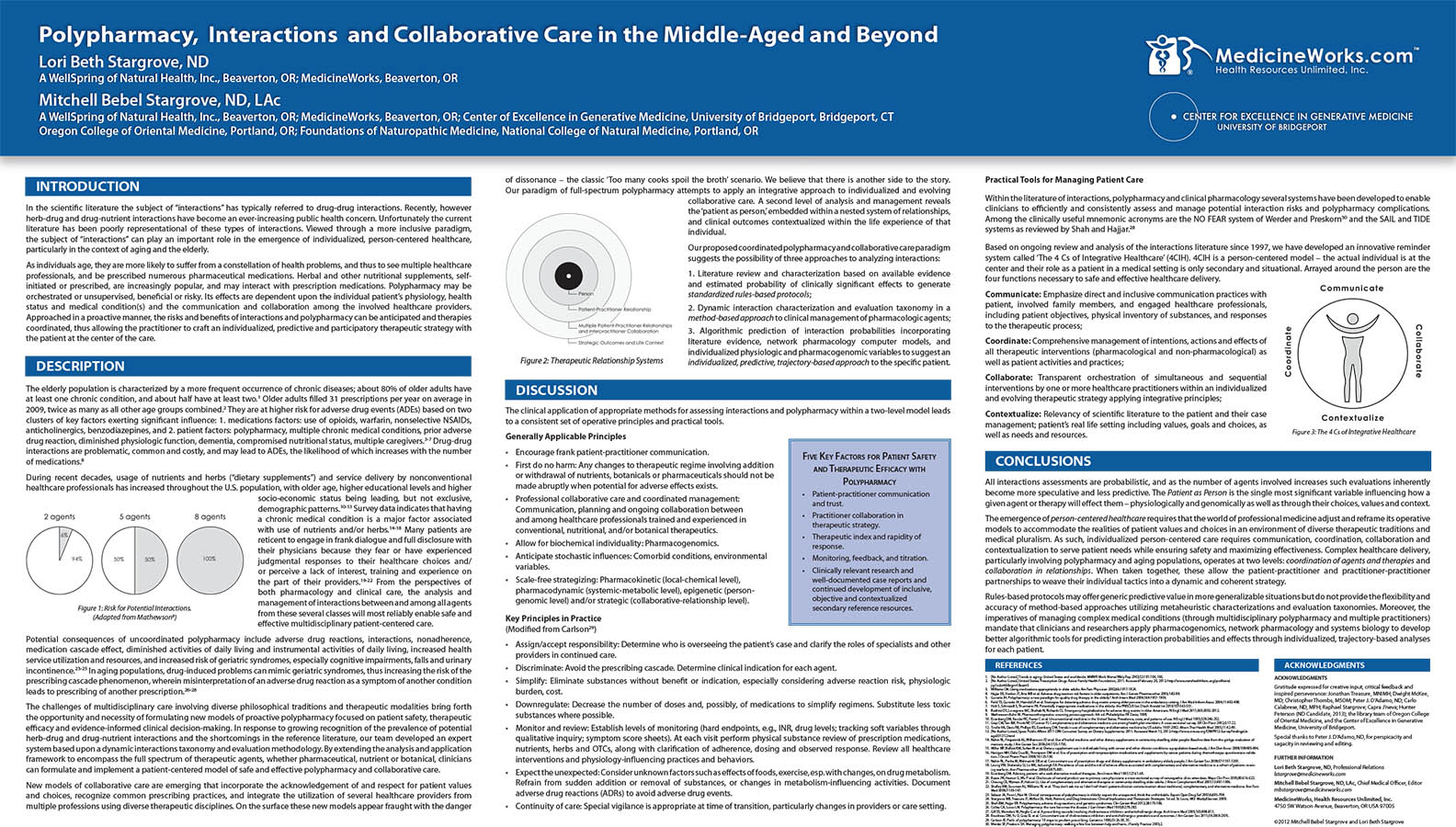
The elderly population is characterized by a more frequent occurrence of chronic diseases; about 80% of older adults have at least one chronic condition, and about half have at least two.1 Older adults filled 31 prescriptions per year on average in 2009, twice as many as all other age groups combined.2 They are at higher risk for adverse drug events (ADEs) based on two clusters of key factors exerting significant influence: 1. medications factors: use of opioids, warfarin, nonselective NSAIDs, anticholinergics, benzodiazepines, and 2. patient factors: polypharmacy, multiple chronic medical conditions, prior adverse drug reaction, diminished physiologic function, dementia, compromised nutritional status, multiple caregivers.3-7 Drug-drug interactions are problematic, common and costly, and may lead to ADEs, the likelihood of which increases with the number of medications.8
During recent decades, usage of nutrients and herbs (“dietary supplements”) and service delivery by nonconventional healthcare professionals has increased throughout the U.S. population, with older age, higher educational levels and higher socio-economic status being leading, but not exclusive, demographic patterns.10-13 Survey data indicates that having a chronic medical condition is a major factor associated with use of nutrients and/or herbs.14-18 Many patients are reticent to engage in frank dialogue and full disclosure with their physicians because they fear or have experienced judgmental responses to their healthcare choices and/or perceive a lack of interest, training and experience on the part of their providers.19-22 From the perspectives of both pharmacology and clinical care, the analysis and management of interactions between and among all agents from these several classes will most reliably enable safe and effective multidisciplinary patient-centered care.
Potential consequences of uncoordinated polypharmacy include adverse drug reactions, interactions, nonadherence, medication cascade effect, diminished activities of daily living and instrumental activities of daily living, increased health service utilization and resources, and increased risk of geriatric syndromes, especially cognitive impairments, falls and urinary incontinence.23-25 In aging populations, drug-induced problems can mimic geriatric syndromes, thus increasing the risk of the prescribing cascade phenomenon, wherein misinterpretation of an adverse drug reaction as a symptom of another condition leads to prescribing of another prescription.26-28
The challenges of multidisciplinary care involving diverse philosophical traditions and therapeutic modalities bring forth the opportunity and necessity of formulating new models of proactive polypharmacy focused on patient safety, therapeutic efficacy and evidence-informed clinical decision-making. In response to growing recognition of the prevalence of potential herb-drug and drug-nutrient interactions and the shortcomings in the reference literature, our team developed an expert system based upon a dynamic interactions taxonomy and evaluation methodology. By extending the analysis and application framework to encompass the full spectrum of therapeutic agents, whether pharmaceutical, nutrient or botanical, clinicians can formulate and implement a patient-centered model of safe and effective polypharmacy and collaborative care.
New models of collaborative care are emerging that incorporate the acknowledgement of and respect for patient values and choices, recognize common prescribing practices, and integrate the utilization of several healthcare providers from multiple professions using diverse therapeutic disciplines. On the surface these new models appear fraught with the danger of dissonance – the classic ‘Too many cooks spoil the broth’ scenario. We believe that there is another side to the story. Our paradigm of full-spectrum polypharmacy attempts to apply an integrative approach to individualized and evolving collaborative care. A second level of analysis and management reveals the ‘patient as person,’ embedded within a nested system of relationships, and clinical outcomes contextualized within the life experience of that individual.
Our proposed coordinated polypharmacy and collaborative care paradigm suggests three possible levels of approaching the categorization, analysis and evaluation of interactions among agents and therapies:
- Literature review and characterization based on available evidence and estimated probability of clinically significant effects to generate standardized rules-based protocols;
- Dynamic interaction characterization and evaluation taxonomy in a method-based approach to clinical management of pharmacologic agents;
- Algorithmic prediction of interaction probabilities incorporating literature evidence, network pharmacology computer models29-33, and individualized physiologic and pharmacogenomic variables to suggest an individualized, predictive, trajectory-based approach to the specific patient.
DISCUSSION
The clinical application of appropriate methods for assessing interactions and polypharmacy within a two-level model leads to a consistent set of operative principles and practical tools.
Generally Applicable Principles
- Encourage frank patient-practitioner communication.
- First do no harm: Any changes to therapeutic regime involving addition or withdrawal of nutrients, botanicals or pharmaceuticals should not be made abruptly when potential for adverse effects exists.
- Professional collaborative care and coordinated management: Communication, planning and ongoing collaboration between and among healthcare professionals trained and experienced in conventional, nutritional, and/or botanical therapeutics.
- Allow for biochemical individuality: Pharmacogenomics.
- Anticipate stochastic influences: Comorbid conditions, environmental variables.
- Scale-free strategizing: Pharmacokinetic (local-chemical level), pharmacodynamic (systemic-metabolic level), epigenetic (person-genomic level) and/or strategic (collaborative-relationship level).
Key Principles in Practice
(Modified from Carlson34)
- Assign/accept responsibility: Determine who is overseeing the patient’s case and clarify the roles of specialists and other providers in continued care.
- Discriminate: Avoid the prescribing cascade. Determine clinical indication for each agent.
- Simplify: Eliminate substances without benefit or indication, especially considering adverse reaction risk, physiologic burden, cost.
- Downregulate: Decrease the number of doses and, possibly, of medications to simplify regimens. Substitute less toxic substances where possible.
- Monitor and review: Establish levels of monitoring (hard endpoints, e.g., INR, drug levels; tracking soft variables through qualitative inquiry; symptom score sheets). At each visit perform physical substance review of prescription medications, nutrients, herbs and OTCs, along with clarification of adherence, dosing and observed response. Review all healthcare interventions and physiology-influencing practices and behaviors.
- Expect the unexpected: Consider unknown factors such as effects of foods, exercise, esp. with changes, on drug metabolism. Refrain from sudden addition or removal of substances, or changes in metabolism-influencing activities. Document adverse drug reactions (ADRs) to avoid adverse drug events.
- Continuity of care: Special vigilance is appropriate at time of transition, particularly changes in providers or care setting.
Practical Tools for Managing Patient Care
Within the literature of interactions, polypharmacy and clinical pharmacology several systems have been developed to enable clinicians to efficiently and consistently assess and manage potential interaction risks and polypharmacy complications. Among the clinically useful mnemonic acronyms are the NO FEAR system of Werder and Preskorn35 and the SAIL and TIDE systems as reviewed by Shah and Hajjar.28
Click image for larger view.
Coordinate: Comprehensive management of intentions, actions and effects of all therapeutic interventions (pharmacological and non-pharmacological) as well as patient activities and practices;
Collaborate: Transparent orchestration of simultaneous and sequential interventions by one or more healthcare practitioners within an individualized and evolving therapeutic strategy applying integrative principles;
Contextualize: Relevancy of scientific literature to the patient and their case management; patient’s real life setting including values, goals and choices, as well as needs and resources.
Five Key Factors for Patient Safety and Therapeutic Efficacy with Polypharmacy
- Patient-practitioner communication and trust.
- Practitioner collaboration in therapeutic strategy.
- Therapeutic index and rapidity of response.
- Monitoring, feedback, and titration.
- Clinically relevant research and well-documented case reports and continued development of inclusive, objective and contextualized secondary reference resources.
CONCLUSION
All interactions assessments are probabilistic, and as the number of agents involved increases such evaluations inherently become more speculative and less predictive. The Patient as Person is the single most significant variable influencing how a given agent or therapy will effect them – physiologically and genomically as well as through their choices, values and context.
The emergence of person-centered healthcare requires that the world of professional medicine adjust and reframe its operative models to accommodate the realities of patient values and choices in an environment of diverse therapeutic traditions and medical pluralism. As such, individualized person-centered care requires communication, coordination, collaboration and contextualization to serve patient needs while ensuring safety and maximizing effectiveness. Complex healthcare delivery, particularly involving polypharmacy and aging populations, operates at two levels: coordination of agents and therapies and collaboration in relationships. When taken together, these allow the patient-practitioner and practitioner-practitioner partnerships to weave their individual tactics into a dynamic and coherent strategy.
Rules-based protocols may offer generic predictive value in more generalizable situations but do not provide the flexibility and accuracy of method-based approaches utilizing metaheuristic characterizations and evaluation taxonomies. Moreover, the imperatives of managing complex medical conditions (through multidisciplinary polypharmacy and multiple practitioners) mandate that clinicians and researchers apply systems biology, pharmacogenomics and network pharmacology to develop better algorithmic tools for predicting interaction probabilities and effects through individualized, trajectory-based analyses for each patient.
REFERENCES
1. [No Author Listed.] Trends in aging–United States and worldwide. MMWR Morb Mortal Wkly Rep 2003;52:101-104, 106.
2. [No Author Listed.] United States: Prescription Drugs. Kaiser Family Health Foundation, 2011. Accessed February 20, 2012: http://www.statehealthfacts.org/profileind.jsp?sub=66&rgn=1&cat=5
3. Willlams CM. Using medications appropriately in older adults. Am Fam Physician 2002;66:1917-1924.
4. Hajjar ER, Hanlon JT, Artz MB et al. Adverse drug reaction risk factors in older outpatients. Am J Geriatr Pharmacother 2003;1:82-89.
5. Gurwitz JH. Polypharmacy: a new paradigm for quality drug therapy in the elderly? Arch Intern Med 2004;164:1957-1959.
6. Field TS, Gurwitz JH, Harrold LR et al. Strategies for detecting adverse drug events among older persons in the ambulatory setting. J Am Med Inform Assoc 2004;11:492-498.
7. Holt S, Schmiedl S, Thurmann PA. Potentially inappropriate medications in the elderly: the PRISCUS list. Dtsch Arztebl Int 2010;107:543-551.
8. Budnitz DS, Lovegrove MC, Shehab N, Richards CL. Emergency hospitalizations for adverse drug events in older Americans. N Engl J Med 2011;365:2002-2012.
9. Mathewson-Kuhn M. Pharmacotherapeutics: a nursing process approach. 4th ed. Philadelphia: FA Davis; 1998.
10. Eisenberg DM, Kessler RC, Foster C et al. Unconventional medicine in the United States. Prevalence, costs, and patterns of use. N Engl J Med 1993;328:246-252.
11. Gray CM, Tan AW, Pronk NP, O’Connor PJ. Complementary and alternative medicine use among health plan members. A cross-sectional survey. Eff Clin Pract 2002;5:17-22.
12. Tindle HA, Davis RB, Phillips RS, Eisenberg DM. Trends in use of complementary and alternative medicine by US adults: 1997-2002. Altern Ther Health Med 2005;11:42-49.
13. [No Author Listed.] Ipsos Public Affairs 2011 CRN Consumer Survey on Dietary Supplements; 2011. Accessed March 15, 2012: http://www.crnusa.org/CRNPR12-SurveyFindingsUsage031312.html
14. Nahin RL, Fitzpatrick AL, Williamson JD et al. Use of herbal medicine and other dietary supplements in community-dwelling older people: Baseline data from the ginkgo evaluation of memory study. J Am Geriatr Soc 2006;54:1725-1735.
15. Miller MF, Bellizzi KM, Sufian M et al. Dietary supplement use in individuals living with cancer and other chronic conditions: a population-based study. J Am Diet Assoc 2008;108:483-494.
16. Hanigan MH, Dela Cruz BL, Thompson DM et al. Use of prescription and nonprescription medications and supplements by cancer patients during chemotherapy: questionnaire validation. J Oncol Pharm Pract 2008;14:123-130.
17. Nahin RL, Pecha M, Welmerink DB et al. Concomitant use of prescription drugs and dietary supplements in ambulatory elderly people. J Am Geriatr Soc 2009;57:1197-1205.
18. Leung VW, Shalansky SJ, Lo MK, Jadusingh EA. Prevalence of use and the risk of adverse effects associated with complementary and alternative medicine in a cohort of patients receiving warfarin. Ann Pharmacother 2009;43:875-881.
19. Eisenberg DM. Advising patients who seek alternative medical therapies. Ann Intern Med 1997;127:61-69.
20. Busse JW, Heaton G, Wu P et al. Disclosure of natural product use to primary care physicians: a cross-sectional survey of naturopathic clinic attendees. Mayo Clin Proc 2005;80:616-623.
21. Cheung CK, Wyman JF, Halcon LL. Use of complementary and alternative therapies in community-dwelling older adults. J Altern Complement Med 2007;13:997-1006.
22. Shelley BM, Sussman AL, Williams RL et al. ‘They don’t ask me so I don’t tell them’: patient-clinician communication about traditional, complementary, and alternative medicine. Ann Fam Med 2009;7:139-147.
23. Salazar JA, Poon I, Nair M. Clinical consequences of polypharmacy in elderly: expect the unexpected, think the unthinkable. Expert Opin Drug Saf 2007;6:695-704.
24. Stargrove MB, Treasure JT, McKee DL. Herb, Nutrient, and Drug Interactions: Clinical Implications and Therapeutic Strategies. 1st ed. St. Louis, MO: MosbyElsevier; 2008.
25. Shah BM, Hajjar ER. Polypharmacy, adverse drug reactions, and geriatric syndromes. Clin Geriatr Med 2012;28:173-186.
26. Colley CA, Lucas LM. Polypharmacy: the cure becomes the disease. J Gen Intern Med 1993;8:278-283.
27. Gill SS, Mamdani M, Naglie G et al. A prescribing cascade involving cholinesterase inhibitors and anticholinergic drugs. Arch Intern Med 2005;165:808-813.
28. Boudreau DM, Yu O, Gray SL et al. Concomitant use of cholinesterase inhibitors and anticholinergics: prevalence and outcomes. J Am Geriatr Soc 2011;59:2069-2076.
29. Schmidt BM, Ribnicky DM, Lipsky PE, Raskin I. Revisiting the ancient concept of botanical therapeutics. Nat Chem Biol. 2007 Jul;3(7):360-366.
30. Hopkins AL. Network pharmacology: the next paradigm in drug discovery. Nat Chem Biol. 2008 Nov;4(11):682-690.
31. Tatonetti NP, Ye PP, Daneshjou R, Altman RB. Data-driven prediction of drug effects and interactions. Sci Transl Med. 2012 Mar 14;4(125):125ra31.
32. Gertsch J. Botanical drugs, synergy, and network pharmacology: forth and back to intelligent mixtures. Planta Med. 2011 Jul;77(11):1086-1098.
33. Efferth T, Koch E. Complex interactions between phytochemicals. The multi-target therapeutic concept of physiotherapy. Curr Drug Targets. 2011 Jan;12(1):122-132.
34. Carlson JE. Perils of polypharmacy: 10 steps to prudent prescribing. Geriatrics 1996;51:26-30, 35.
35. Werder SF, Preskorn SH. Managing polypharmacy: walking a fine line between help and harm. J Family Practice 2003;2.
AFFILIATIONS
Lori Beth Stargrove, ND
A WellSpring of Natural Health, Inc. (Beaverton, OR); MedicineWorks (Beaverton, OR)
Mitchell Bebel Stargrove, ND, LAc
A WellSpring of Natural Health, Inc. (Beaverton, OR); MedicineWorks (Beaverton, OR); Center of Excellence in Generative Medicine, University of Bridgeport (Bridgeport, CT), Oregon College of Oriental Medicine, (Portland, OR); Foundations of Naturopathic Medicine, National College of Natural Medicine, (Portland, OR)
ACKNOWLEDGMENTS
Gratitude expressed for creative input, critical feedback and inspired perseverance: Jonathan Treasure, MNIMH; Dwight McKee, MD; Christopher Thombs, MSOM; Peter J. D’Adamo, ND; Carlo Calabrese, ND, MPH; Raphael Stargrove; Capra J’neva; Hunter Peterson (ND Candidate, 2013); the library team of Oregon College of Oriental Medicine; and the Center of Excellence in Generative Medicine, University of Bridgeport.
Special thanks to Peter J. D’Adamo, ND, for perspicacity and sagacity in reviewing and editing.
FURTHER INFORMATION
Lori Beth Stargrove, ND
Chief Health Officer, Professional Relations
Mitchell Bebel Stargrove, ND, LAc
Chief Medical Officer, Editor
MedicineWorks, Health Resources Unlimited, Inc.
4750 SW Watson Avenue, Beaverton, OR USA 97005
©2012 Mitchell Bebel Stargrove and Lori Beth Stargrove
